Surgeon/Restorative dentist:
Dr. Roberto Meli – Florence, Italy
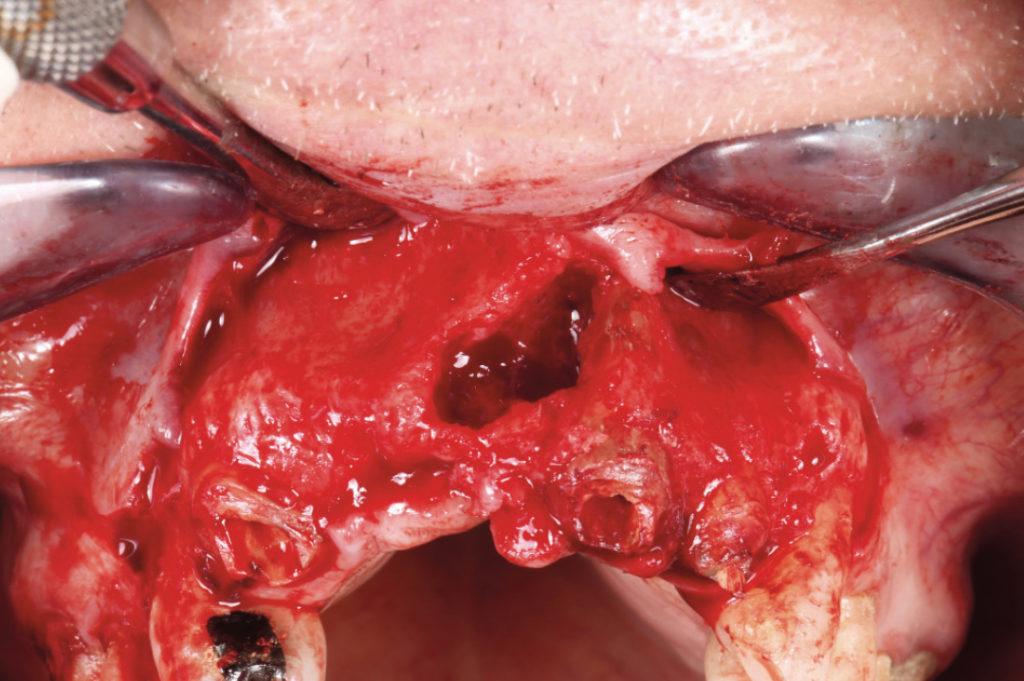
This case shows the treatment of an edentulous maxillary anterior space with severe resorption of the residual ridge. The patient, suffering from diabetes and an autoimmune disorder (Guillain-Barré), asked for a fixed prosthesis without undergoing time consuming surgical procedures. Due to this particular patient situation, a complex bone grafting procedure to regenerate the missing bone volumes was not contemplated. Two 3.75 x 12 mm XCN implants were placed in position #12 and #22 with a two-stage surgical procedure with simultaneous bone graft and a temporary mobile prosthesis was applied. After six months of healing, the implants were uncovered and a screw-retained prosthesis with pink composite resin to mask the severe gingival defect was fabricated. Thanks to this approach not only the teeth but also gingival aesthetics and anatomy were reproduced.

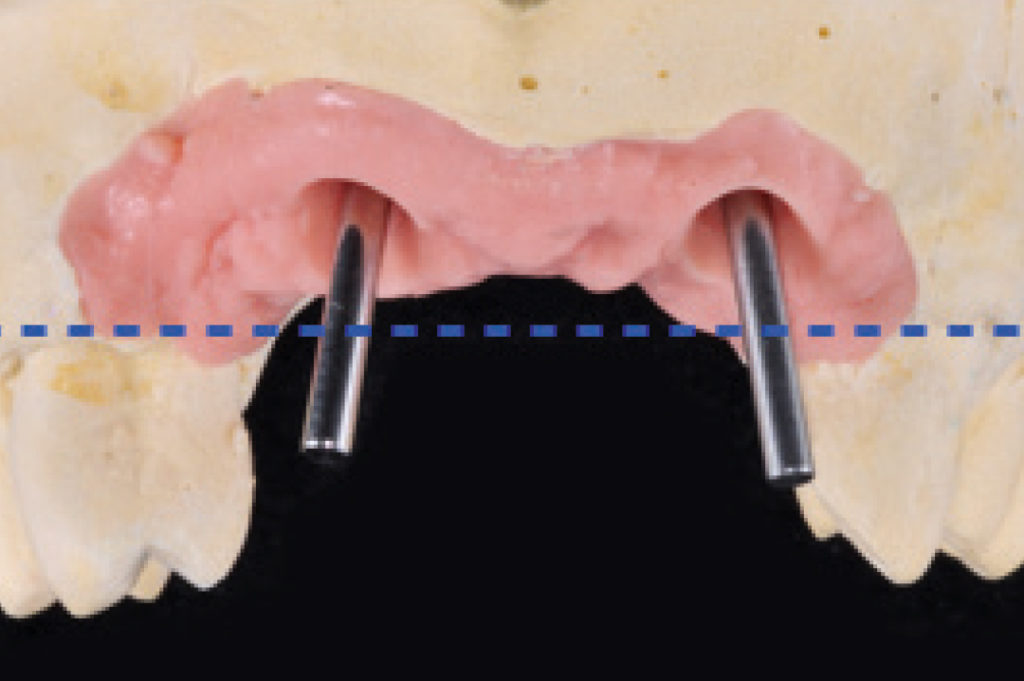
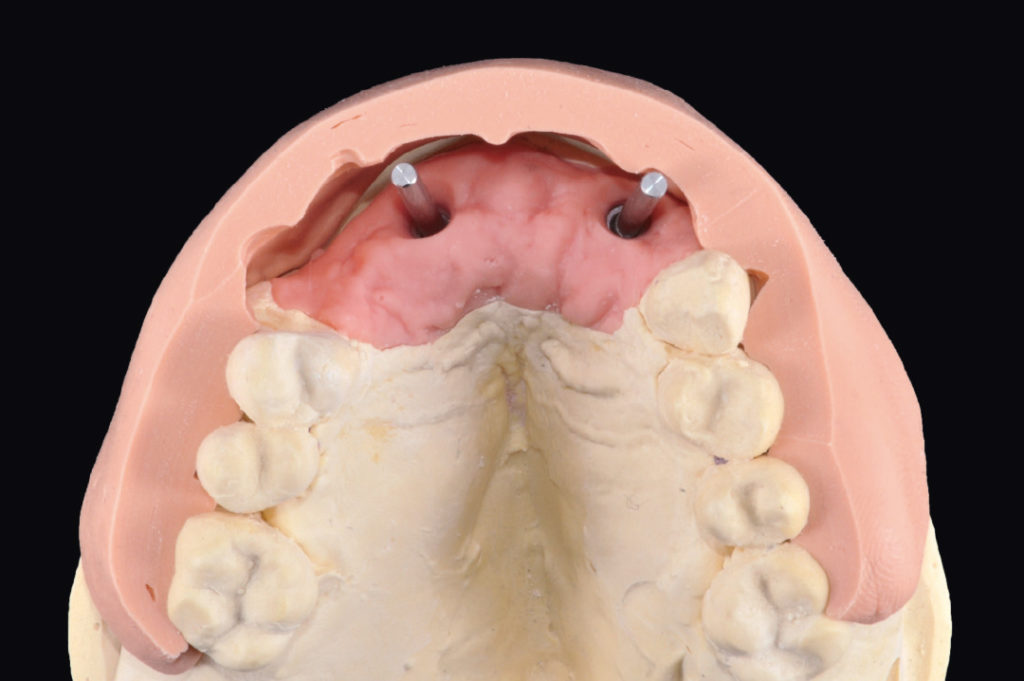
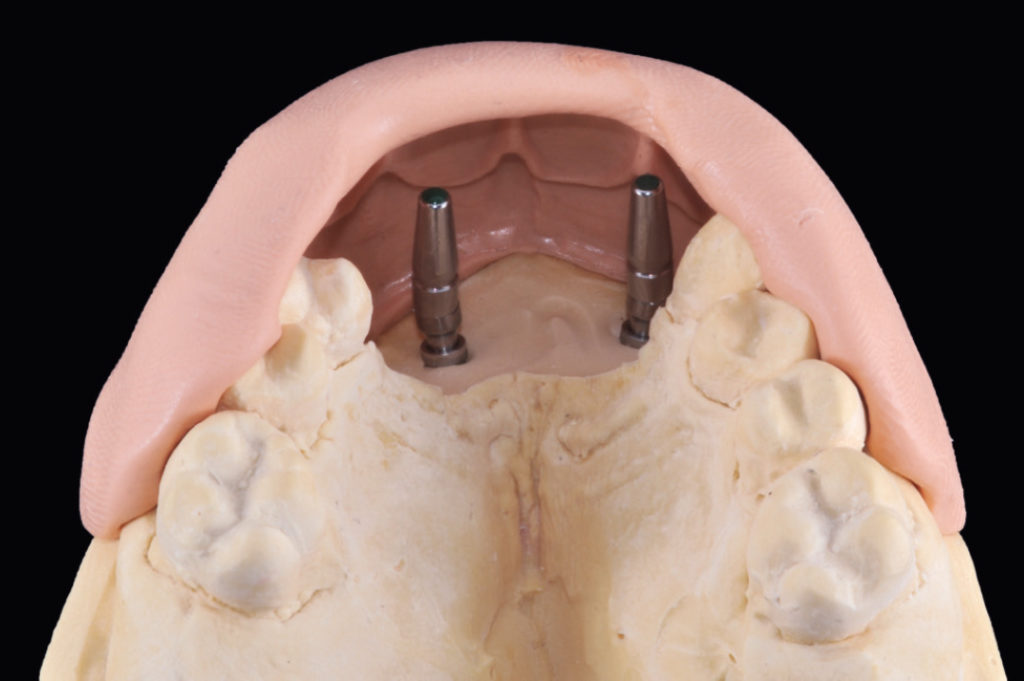
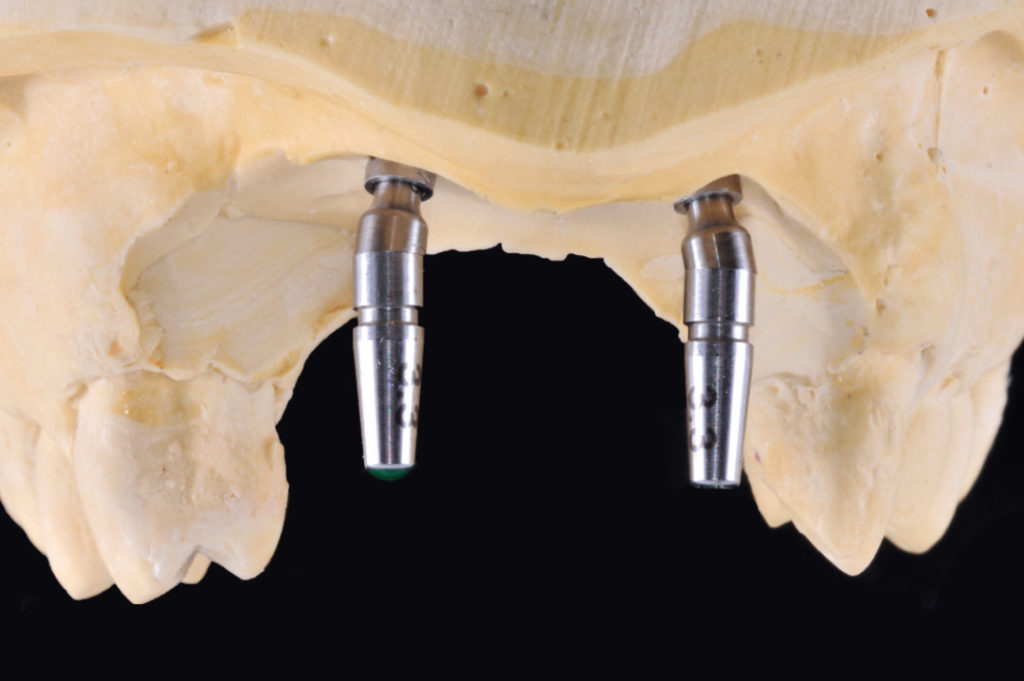
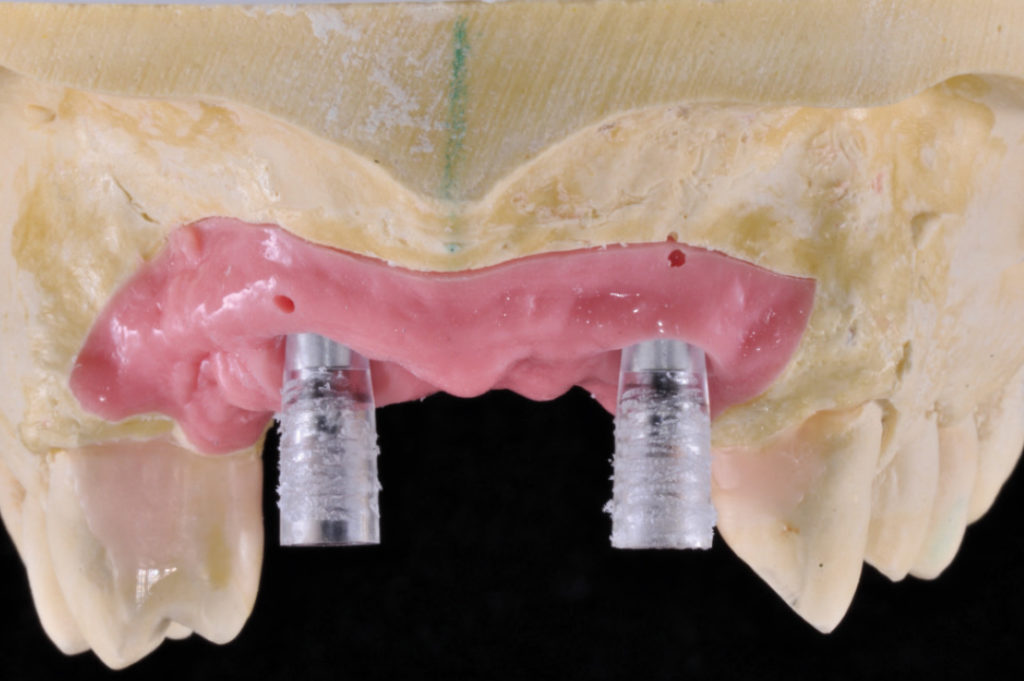
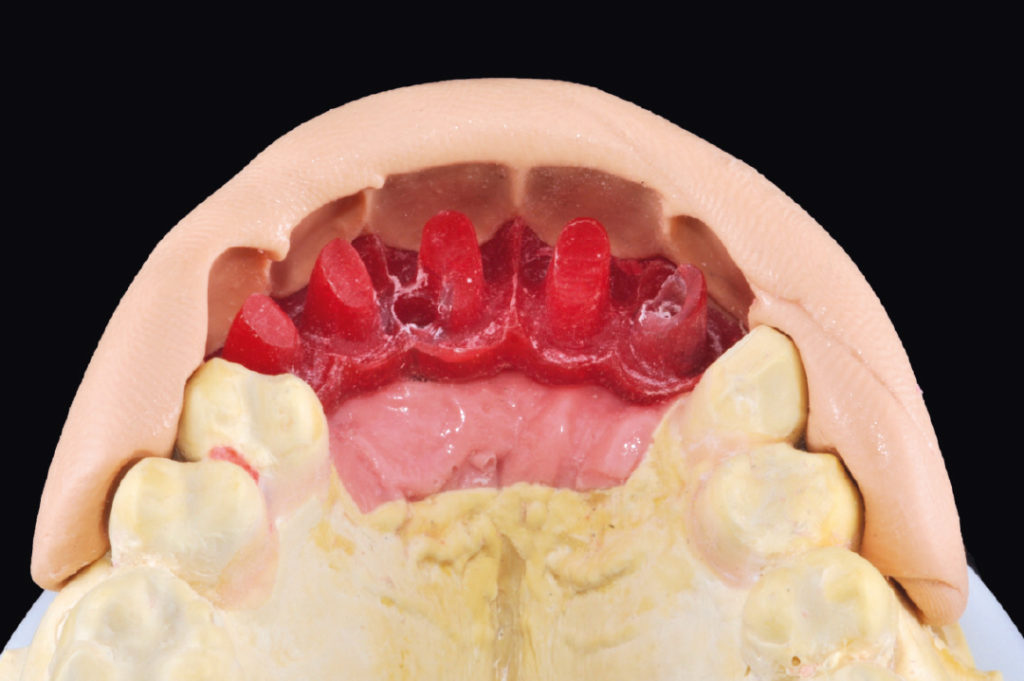
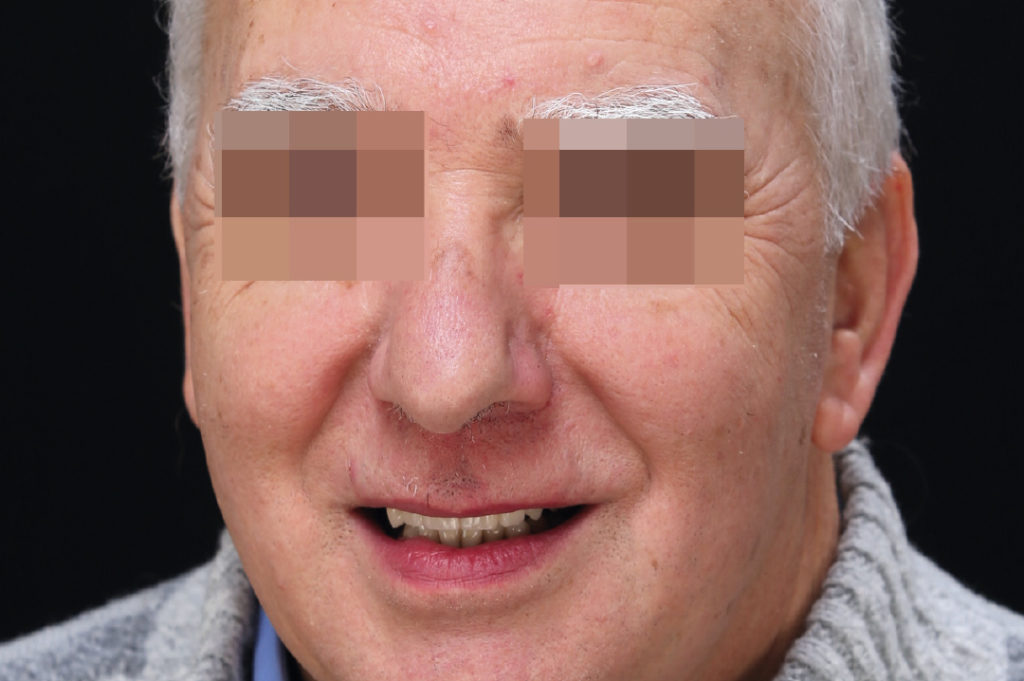
Pre-operative clinical view View of the anterior maxillary area and of the bone defect after flap reflection Temporary mobile prosthesis made from acrylic resin in place Healing caps on two XCN Max Stability implants 3.75 x 12 mm in position #12 and #22 Dental cast after implant-level impression: selection of MUAs Dental cast with silicone key: the space is unequally distributed Diagnostic wax-up Intraoral evaluation of the diagnostic wax-up Dental cast with silicone key: transfers screwed on two 15° angled MUAs GH 1,5 for better grip and visualization; as the apical hexagon is separated from the rest of the abutment, abutments can be rotated to their correct angular position Check of parallelism; once found, the apical hexagon is permanently connected in the selected position to the abutment Definitive seating of MUAs into the implants Transfers screwed onto the abutments for impression taking on abutment-level Transfers placed in the impression High burn-out copings positioned on abutment-analogs within the master cast Fabrication of a pattern resin prototype with “enamelled” teeth to evaluate function and aesthetics Lateral view of pattern resin prototype placed on the master cast of upper and lower jaw Lateral view of pattern resin prototype placed on the master cast of upper and lower jaw Pattern resin prototype Intraoral evaluation of the pattern resin prototype Reduction of the pattern resin prototype Evaluation of the reduced pattern resin frame by means of the silicone key Pattern resin frame ready for casting Try-in of the cast metal structure on the master cast Intraoral try-in of the metal structure Shade selection for pink composite resin to mask the severe gingival defect Sandblasted metal structure Metal structure after application of opaque layers Copings made from castable resin Detached resin copings Monolithic crowns in preparation Finished monolithic crowns Finished structure with polished artificial composite gingiva Prosthesis ready for delivery Try-in of the definitive prosthesis on the master cast Master cast, finished structure with artificial composite gingiva, five single monolithic crowns Finished structure fixed onto the abutments with connecting screws for final try-in Evaluation of aesthetics and ease of cleaning Prosthesis is repositioned on the master cast for the luting of three monolithic crowns onto the finished structure with Multilink Hybrid Abutment bonding composite Prosthesis definitively fixed onto the abutments with connecting screws; screw access holes are sealed Occlusal view of the prosthesis after cementation of the remaining two crowns with temporary cement onto the structure Lateral view of the prosthesis: as the space was unequally distributed (see fig. 6) there is a diastema between teeth #22 and #23 Lateral view of the prosthesis after diastema closure Facial view of the prosthesis Patient’s smile




































Link to the original article published in 2017
Laboratory:
Accioli & Puccini – Florence, Italy